Journal of Infection and Molecular Biology
Research Article
Journal of Infection and Molecular Biology 2 (3): 32 – 34rs 10735810 of Vitamin D Receptor (VDR) Gene : Association with Pulmonary Tuberculosis in Children
Bindi Das Mohandas Sulaja*, Ugam Kumari Chauhan2
-
Centre for Biotechnology Studies, A.P.S University, Rewa, MP, India
*Corresponding author: bindidas_ms@yahoo.com
ARTICLE CITATION:
Sulaja BDM, Chauhan UK (2014). rs 10735810 of vitamin d receptor (VDR) gene: association with pulmonary tuberculosis in children. J. Inf. Mol. Biol. 2 (3): 32 – 34.
Received: 2014–03–27, Revised: 2014–04–21, Accepted: 2014–04–23
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/jimb.2307-5465/2.3.32.34
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Tuberculosis (TB) in children is an important cause of morbidity and mortality worldwide. There is much risk of severe disease and death among young than adults, therefore, the pediatric tuberculosis remains a public health emergency. Vitamin D receptor (VDR) mediates the immunological function of vitamin D3 which activates macrophages and its deficiency concerned to the risk of TB. So polymorphisms in VDR gene may influence the function of vitamin D and susceptibility to TB. This study is to investigate the existence of possible association between VDR Fok I polymorphism (rs 10735810) and pediatric pulmonary tuberculosis in Madhya Pradesh of central India, using polymerase chain reaction-restriction fragment length polymorphism (PCR - RFLP). The VDR Fok I polymorphism showed statistically significant association with pediatric pulmonary TB in central Indian population. The FF genotype and F allele showed lower risk to TB in children while the heterozygous Ff genotype could be associated with pathophysiology of pediatric TB (OR = 2.413). The ff genotype was statistically non-significant as the frequency of this genotype was very less in both cases (5.97%) and control (2.5%).
INTRODUCTION
Children are more likely to develop disease from a recent infection thus pediatric tuberculosis often reflects recent TB transmission within a community and consequently provides useful markers for monitoring and directing TB control programs (Reinhard et al., 1997). Many single-nucleotide polymorphisms (SNPs) have no effect on cell function, but some SNPs, especially if they affect the function of the gene, could predispose people to disease or influence their response to a drug (Sachidanandam et al., 2001). Significant associations between tuberculosis and gene polymorphisms have been studied in different populations, of which VDR polymorphism thought to be important due to its role in immune system and different studies reported that VDR Fok I polymorphism is associated with TB in North Central Indians (Sharma et al., 2011), Chinese (Wei et al., 2009) and South Indians (Selvaraj et al., 2003). So this work was conducted to study the association of Fok 1 VDR gene polymorphisms with genotype frequencies, allele frequencies and carriage rate distribution in patients with pulmonary tuberculosis among central Indian population to determine the association with pediatric tuberculosis.
VDR, a nuclear hormone receptor, is a member of the steroid receptor family present on monocytes and activated T and B lymphocytes (Provvedini et al., 1983) involved in a wide range of biological functions, including mediation of vitamin D3 interactions with the immune system (Rostand et al., 2008). Vitamin D is a critical immunoregulatory factor in inhibiting engulfed Mycobacterium from surviving in macrophage as its metabolism is closely related to macrophage activation (Manolagas et al., 1994). Vitamin D3-VDR complex regulates the production of cathelicidin and defencin, two antimicrobial peptides, by the interaction with vitamin D response elements (VDRE) present on the promoter of cathelicidin and defencin genes (Nizet et al., 2001). Cathelicidin and defencin disrupt the integrity of the bacterial cell membrane resulting the death of the microbe (Ganz, 2004). So polymorphisms in the VDR gene may be a contributing factor to increase tuberculosis susceptibility. Fok I creates an alternative initiation codon (ATG), three codon from length by three amino acids, and the transcription of this allele is 1 - 7 times less efficient than the F allele, and can alter the amount of VDR produced (Uitterlinden et al., 2004).
MATERIALS AND METHODS
Study population
The study population consisted of 134 pulmonary TB patients (age > 14. Male - 60, Female - 73) and 160 controls from central India. Control subjects matched with patients by age (> 14), sex (Male - 74, Female - 87) and ethnicity (Central India).
Isolation of genomic DNA from blood samples
Genomic DNA was extracted from whole blood by the modification of salting out procedure described by Miller and coworkers (Miller et al., 1988).
VDR Genotyping by PCR - RFLP
The Fok I region was amplified using forward primer 5′- AGCTGGCCCTGGCACTGACTCTGCTCT -3′ and reverse primer 5′- AGGAAACACCTTGCTTCTTCTCCCTC -3′ under the thermal conditions as follows: initial denaturation at 940 C for 3min followed by 35 cycles of denaturation at 940 C for 1 min, annealing at 600 C for 1 min, and extension at 720C for 1 min. The final extension was carried out for 3 min. Lambda DNA EcoRІ double digest (Bangalore Genei, Bangalore, India) was used as molecular weight marker. Ladder with amplified product has been run on 1% agarose gel.
The PCR products were digested with Fok I (New England Biolabs, USA). The resultant products were analyzed on 2% agarose gel stained with ethidium bromide. A 1000 bp gene DNA ladder (Roche, Germany) was run concurrently as molecular weight marker. The products were visualized using an ultraviolet trans-illuminator. Fok I was amplified following the protocol described by Babb et al (2007).
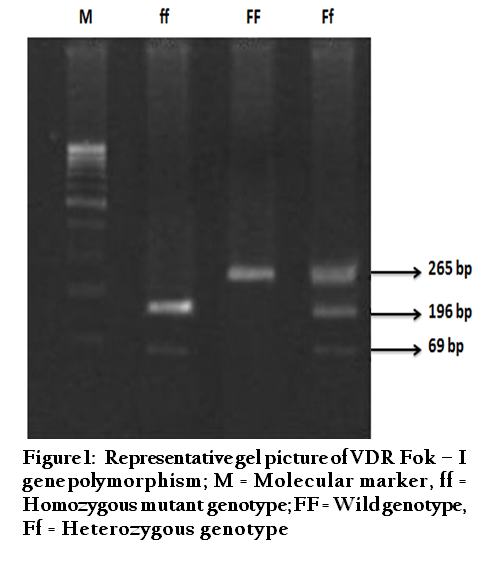
Based on the Fok I cleavage pattern VDR genotype was determined as FF (presence of an uncleaved 265 bp product which represents the gene is homozygous for absence of restriction site), ff (shows two fragments of 196 bp and 69 bp which represents the gene is homozygous for presence of restriction site) and Ff (shows three fragments of 196 bp, 69 bp and 265 bp which represents the gene is heterozygous for restriction site) (Figure 1).
Statistical Analysis
Prism 5.0, San Diego, USA (www.graphpad.com) was used for statistical analysis.
RRESULT
The distribution of VDR-Fok I polymorphism (rs 10735810) was consistent with Hardy Weinberg equilibrium (HWE) in TB patients as well as in control subjects.
VDR- Fok I genotype distribution was significantly different in healthy control group with respect to TB disease group (table I). The common genotype (FF) was high in healthy control subjects than patients (71.87% vs. 60.45%). The odds ratio of FF genotype is 0.5449 shows its protective effect. The mutant genotype ff was less in TB patients (5.97%) as well as in control group (2.5%). The heterozygous Ff genotype was higher in patients (33.58%) with respect to control group (23.12%) and had an odds ratio of 1.626 and P value of 0.0682, the odds ratio advocates that it could be associated with pathophysiology of pediatric TB in the study population.

The frequency of allele F was lower in TB patients (77.24%) with respect to the case group (83.44%) whereas the f allele is higher in TB patients (22.76%) than control group (14.06%) (χ2 = 6.711; P = 0.0096). The odds ratio of F allele was 0.5719 which indicates its protective role. The carriage rate of F allele was not different in patients and healthy subjects while the f allele was higher in TB patients with respect to control (χ2 =3.442; P = 0.0636) but the values are non-significant even though the f allele shows an odds ratio of 0.6413. The frequency of FF genotype and F allele were higher in healthy controls which designates it has low risk (P = 0.0173; OR = 0.5449, 95% CI 0.314 - 0.8958 and P = 0.0129; OR = 0.5719, 95% CI 0.3736 - 0.8756 respectively).
DISCUSSION
Vitamin D status appears to be involved in the activation of macrophages and restricts the intracellular growth of mycobacteria (Vidyarani et al., 2007). This effect of vitamin D may be influenced by polymorphisms in the VDR gene (Haussler et al., 1998). Many studies suggest that single nucleotide polymorphisms (SNP) in the VDR gene are associated with TB in different populations (Roth et al., 2004). Therefore, we studied the association between VDR Fok I polymorphism and pediatric pulmonary tuberculosis in Central Indian population. In our study the subjects with FF genotype and F allele show less risk to TB while the odds ratio of Ff (OR = 1.626) genotype suggests that it could be associated with the pathophysiology of pediatric TB and ff genotype was not associated with TB as it was not frequently observed among both TB patients (5.97 %) and control subjects (2.5%).
Our study results are supported by the report of (Sharma et al., 2011), in general population from North-Central India, the subjects with FF genotype of Fok I polymorphism appeared less likely (p = 0.004) to develop MDR TB whereas, those with Ff and ff genotypes were at high risk of MDR and smear positive disease, respectively. In both studies FF genotype didn’t show susceptibility to TB. Ff genotype did show susceptibility to TB in the study of (Sharma et al., 2011) but in our study it could be associated with pathophysiology of pediatric TB. While in the above mentioned study ff genotype showed susceptibility but in our study the ff genotype was not observed frequently either in patients or in control subjects
In the present study the F allele have shown protective role (OR = 0.5719) this was supported by the reports of (Alicia et al., 2007), reported their results had indicated that among the Ache (indigenous population from stern Paraguay) Fok I F allele of VDR gene protects individuals from mycobacterial infection, and (Wibur et al., 2007), reported the Fok I F allele associated with protection against infection in a large-scale genetic analysis of native South Americans. The VDR gene with FF genotype demonstrated an increased transcription rate and this has provided the main explanation for association between Fok I genotype and the development of diseases. Moreover, the production of vitamin D level may change depending on the environment as well as exposure to sunlight (ultraviolet rays).
Studies in South Indian pulmonary TB patients on Fok I polymorphisms of VDR gene showed an increased frequency of the genotype FF (homozygote) in male patients suggested the association with the susceptibility to TB (Selvaraj et al., 2003). The different results shown by Central Indian and South Indian populations may be due to the diversity of these two Indian populations and their difference in origins ( Papiha, 1996). Wei et al. (2009) reported no association was found between VDR polymorphisms (either allele or genotype) and susceptibility to paediatric TB in the Chinese Han population. These reports suggest that the different effects of VDR genotypes in different ethnic populations may be due to gene–environment and gene–gene interactions. However, the internal relation between the environment and the host gene is unknown but it will help to explain the heterogenicity observed in studies and it should be addressed as an influencing factor for future studies. The polymorphic variants of VDR gene along with other gene and environmental factors may be responsible for an altered cell-mediated immunity against M. tuberculosis in a susceptible or resistant host.
Although several investigators reported and suggested that the VDR polymorphism may be of immune-regulatory significance for TB but it is not clear that the polymorphism determine susceptibility to the development of clinical disease or susceptibility to infection. Further studies will be required to explore how VDR polymorphism may influence susceptibility to infectious disease or development of clinical disease.
ACKNOWLEDGMENTS
I would like to express my deepest sense of gratitude to my supervisor Prof. Smt. U. K. Chauhan, Professor and Head School of Environmental Biology, APS University, who offered her continuous advice and encouragement throughout the course of this work. My sincere thanks to Dr. Sunil Rao, Associate Professor of Department of Pediatrics, S. S. Medical College Rewa, and Dr. Sandeep Bhagat, Block Medical Officer, Rampur Naikin, District Sidhi, for helping me in collection of Blood samples and clinical diagnosis. Thanks are due to Dr. Lal Patholab, Ranbaxy Patholab, Krishna Pathology and mothers who were covered in this study, for voluntarily providing me the blood samples of their children to complete this work.
REFERENCES
Alicia K, Kubatko LS, Hurtado AM, Hill KR, Stone AC (2007). Vitamin D receptor gene polymorphisms and susceptibility M. tuberculosis in Native Paraguayans. Tuberculosis. 87: 329 - 337.
http://dx.doi.org/10.1016/j.tube.2007.01.001
PMid:17337247
Babb C, Van Der ML, Beyers N (2007). Vitamin D receptor gene polymorphisms and sputum conversion time in pulmonary tuberculosis patients. Tuberculosis (Edinb).87: 295 – 302.
http://dx.doi.org/10.1016/j.tube.2007.03.001
PMid:17449323
Ganz T (2004). Defensins: antimicrobial peptides of vertebrates. C. R. Biol. 327(6): 539 – 549.
http://dx.doi.org/10.1016/j.crvi.2003.12.007
PMid:15330253
Haussler MR, Whitfield GK, Haussler CA, Hsieh JC (1998). The nuclear vitamin D receptor: biological and molecular regulatory properties revealed. J. Bone. Miner. Res. 13: 325 – 349.
http://dx.doi.org/10.1359/jbmr.1998.13.3.325
PMid:9525333
Wei J, ZhaoNa L, Lin S, ShunYing Z (2009). Vitamin D receptor gene polymorphisms and susceptibility to pediatric tuberculosis among the Chinese population. Chinese J. Prac. Pediatrics. 24 (4): 264 - 266.
Manolagas SC, Yu XP, Girasole G, Bellido T (1994). Vitamin D and the hemato-lymphopoietic tissue: a 1994 update. Semin. Nephrol. 14(2):129 - 43.
PMid:8177980
Miller SA, Dykes DD, Polesky HF (1988). A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 16: 1215.
http://dx.doi.org/10.1093/nar/16.3.1215
PMid:3344216 PMCid:PMC334765
Nizet V, Ohtake T, Lauth X (2001). Innate antimicrobial peptide protects the skin from invasive bacterial infection. Nature. 414: 454 –457.
http://dx.doi.org/10.1038/35106587
PMid:11719807
Papiha SS (1996). Genetic variation in India. Human Biol. 68(5): 607 - 628.
PMid:8908794
Provvedini DM, Tsoukas CD, Deftos LJ, Manolagas SC (1983). Dihydroxyvitamin D3 receptors in human leukocytes. Science. 221: 1181 - 83.
http://dx.doi.org/10.1126/science.6310748
PMid:6310748
Reinhard C, Paul WS, Mcauley JB (1997). Epidemiology of pediatric tuberculosis in Chicago, 1974 to 1994: a continuing public health problem. Am. J. Med. Sci. 313:336 – 340.
http://dx.doi.org/10.1097/00000441-199706000-00004
PMid:9186147
Rostand SG, Warnock DG (2008). Introduction to Vitamin D Symposium, March 14, 2008. Clin. J. Am. Soc. Nephrol. 3: 1534.
http://dx.doi.org/10.2215/CJN.01130308
PMid:18400968
Roth DE, Soto G, Arenas F (2004). Association between vitamin –D receptor gene polymorphisms and response to treatment of pulmonary tuberculosis. J. Infect. Diseases. 920 - 927.
http://dx.doi.org/10.1086/423212
PMid:15295697
Sachidanandam R, Weissman D, Schmidt SC (2001). A map of human genome sequence variation containing 1.42 million single nucleotide polymorphisms. Nature 409: 928 – 933.
http://dx.doi.org/10.1038/35057149
PMid:11237013
Selvaraj P, Chandra G, Kurian SM, Reetha AM (2003). Association of vitamin D receptor gene variants of BsmI, ApaI and FokI polymorphisms with susceptibility or resistance to pulmonary tuberculosis. Curr. Sci. 84: 1564 – 1568.
Sharma PR, Singh S, Jena M, Mishra G (2011). Coding and non-coding polymorphisms in VDR gene and susceptibility to pulmonary tuberculosis in tribes, castes and Muslims of Central India. Infect. Genet. Evol. 11(6):1456 - 1461.
http://dx.doi.org/10.1016/j.meegid.2011.05.019
PMid:21645645
Uitterlinden AG, Fang Y, van Meurs JB (2004). Gene Genetics and biology of vitamin D receptor polymorphisms. Gene 338: 143 – 156
http://dx.doi.org/10.1016/j.gene.2004.05.014
PMid:15315818
Vidyarani M, Selvaraj P, Jawahar MS, Narayanan PR (2007). 1, 25 Dihydroxyvitamin D3 modulated cytokine response in pulmonary tuberculosis. Cytokine. 40: 128 – 134.
http://dx.doi.org/10.1016/j.cyto.2007.08.005
PMid:17911026
Wilbur AK, Kubatko LS, Hurtado AM (2007). Vitamin D receptor gene polymorphisms and susceptibility M. Tuberculosis in native Paraguayans. Tuberculosis. 87: 329 – 37.
http://dx.doi.org/10.1016/j.tube.2007.01.001
PMid:17337247